Insight
Audiological diagnosis and management of glue ear
Written by Scott Drummond · 14 April 2026 · 7 min read
Scott Drummond on how glue ear (otitis media with effusion) is diagnosed and managed — the signs to look for, the tests we use, and the treatment options for children.

Otitis media with effusion (OME), also known as "glue ear," is the most common cause of hearing impairment in children, with children under five years most affected. OME can cause temporary hearing loss and delayed speech development, and may impact behaviour and educational progress.
OME occurs when fluid builds up in the middle ear cavity. This is often, but not always, linked to ear infections. Fluid build-up can occur as a result of Eustachian tube inflammation, which can prevent air getting to the middle ear. With no ventilation, the lining of the middle ear starts to produce fluid — and in turn OME. In children the Eustachian tube is not as wide or as vertical as in adults, so they are more prone to blockage.
Diagnosis and when to refer
Patients with OME will normally present in the clinic as a result of parental or school concern. On taking a history, parents may complain that their child misunderstands instructions, asks for things to be repeated, or is not developing speech as expected.
Parents may sometimes be unaware of a problem, and school may have highlighted hearing as an issue in class, or the child may have failed a school hearing screening test. OME can present with symptoms similar to those seen in other conditions, such as behaviour problems, poor progress at school or speech and language problems. It is therefore important that OME is not overlooked and that otoscopy is carried out.
When performing otoscopy, identification of abnormalities in the shape of the tympanic membrane (TM) is a good indicator of OME. The drum may be bulging or retracted inwards. The colour is also important; the normal drum is quite translucent and a "light reflex" can be observed. If OME is present the drum can look yellow or darker than normal with no light reflex, and fluid bubbles can sometimes be seen behind the drum. In some cases OME can be very difficult to identify through otoscopy alone, due to only slight changes in the TM appearance.
If OME is suspected, further tests should be carried out with an audiologist to confirm diagnosis and assess impact on hearing levels. Audiological tests will include Pure Tone Audiometry (PTA) to assess the extent of hearing loss, and tympanometry to measure middle ear function. The following case study gives an example of how both these tests are used to identify OME.
Case study
Parents of patient "EE" (aged 2.5 years) were concerned as his speech was not developing as quickly as his older brother's. EE also speaks loudly and had recently shown signs of frustration and anxiety at nursery. Otoscopy indicated slight reddening of the eardrum, with a retraction of the TM. EE was thought to have possible glue ear and was referred for audiological testing.
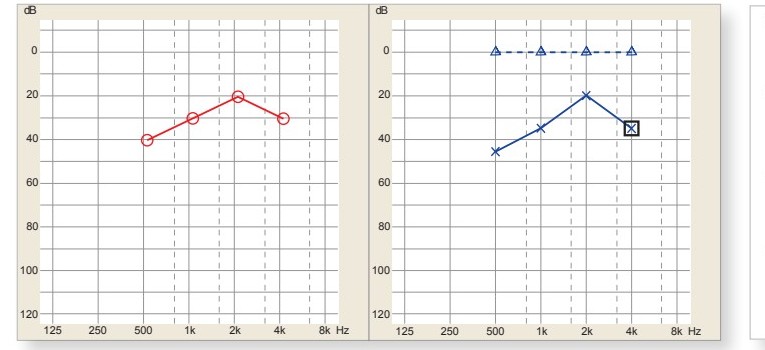
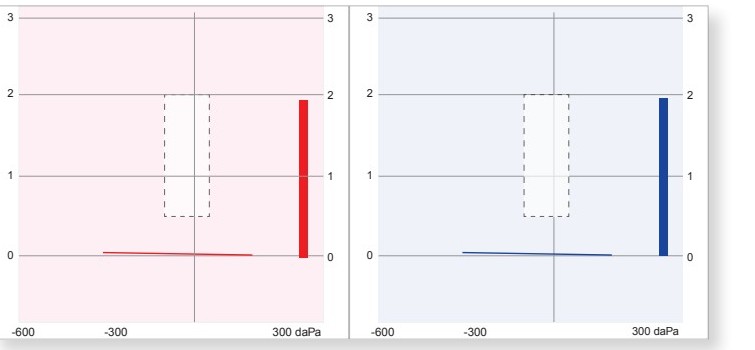
Audiological testing consisted of pure tone audiometry and tympanometry. PTA indicated a bilateral mild conductive hearing loss, and tympanometry showed a type B flat tympanogram. The conductive nature of the hearing impairment and the flat tympanogram confirmed the diagnosis of OME. The PTA results also suggested that the glue ear had reduced hearing to a level sufficient to affect speech development — so management options needed to be considered for EE.
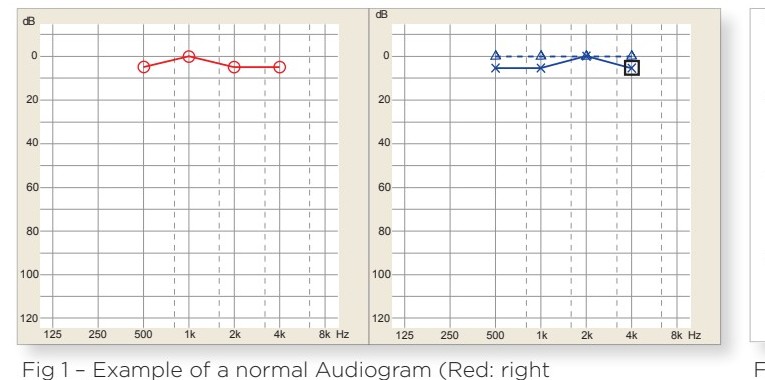
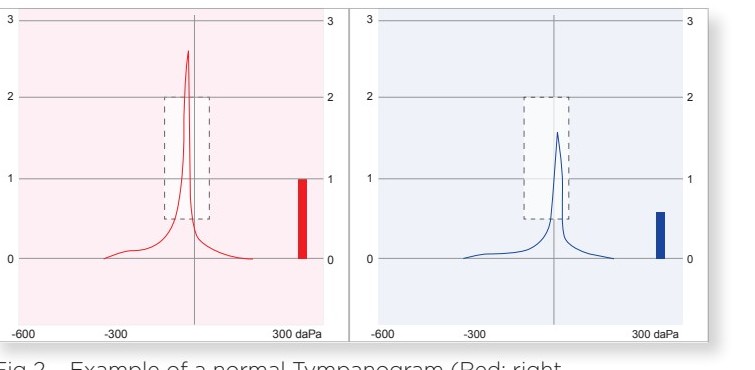
Normal results (for comparison)
EE's test results
Management
In most cases OME will resolve of its own accord within the first three months of diagnosis, and so a policy of "active observation" is recommended (NICE guidelines) with no immediate treatment. After three months, another audiological examination is advised to confirm whether OME has resolved.
Together with active observation, autoinflation using an "Otovent" may help. This involves the child blowing up a special balloon with their nose, which in turn increases pressure in the nose and helps clear the Eustachian tube. The Otovent has varying degrees of success, and a follow-up audiological assessment is still required. Clearing the Eustachian tube has in the past also been attempted using antihistamines, decongestants and steroid sprays — however, research suggests these medical treatments have little or no effect on shortening the duration of OME, and can cause side effects.
Persistent OME lasting longer than a minimum of three months, with adverse effects on the child's hearing, may require further surgical management with an ENT consultant. Grommet surgery involves draining fluid and inserting tubes in the eardrum to ventilate the middle ear. After grommet insertion a follow-up audiological examination is carried out to reassess hearing levels, and in most cases hearing improves to normal. Grommets are not permanent and over time will fall out, so it's important to monitor hearing levels even after the initial post-operative assessment. Grommet insertion is the most common and effective treatment for OME; if surgery is not an option, then hearing aids for the duration of the OME can be an effective management strategy.
Related reading: What is earwax? Why we have it, and when it needs removing.
Concerned about your child's hearing?
Scott offers full paediatric audiological assessment — including pure tone audiometry, tympanometry and a written audiological report — at the Bupa Cromwell Hospital in Kensington.
Book an appointmentThis article is for general information and isn't a substitute for individual medical advice.